The exact process of treating trauma will vary depending on what type of trauma therapy techniques your therapist uses, such as CPT or EMDR. If you’re seeking co-occurring treatment for trauma-related substance use, you’ll follow a few general steps, though your treatment will be personalized to your specific needs. Below are the typical steps for treating substance use and trauma:
The first step in treating trauma that occurs alongside substance use disorders is to detox from alcohol or drugs so you can focus on your treatment. You may participate in a medication-assisted treatment program to help you handle the withdrawal symptoms and prevent relapse as you go through the rest of your personalized treatment program.
These medications help block the effects of different substances or trick your brain into thinking that you’re still taking these substances, so you don’t experience severe withdrawal or feel tempted to turn back to drugs and alcohol.
As you go through detox, you’ll participate in group or individual therapy, including trauma-focused therapy and other types of treatment. As the substance leaves your body, your physical and mental health can improve, which will help you focus on your treatment.
Since trauma can be found at the root of many individuals’ addictions, it’s beneficial to go through the necessary treatments to address your experiences and reduce your responses to them. Trauma-informed therapy helps you process your trauma and there are various types of this therapy that your therapist may offer.
For example, you may participate in prolonged exposure therapy if you have avoidance behaviors or EMDR if you have trouble processing your traumatic responses and memories.
Your therapist helps you determine what type of therapy would work best by performing an assessment to get a baseline for your past experiences, current struggles and goals. Based on this information, you’ll work together to determine what type of therapy can work best.
You’ll likely also participate in other therapy to address your substance use, such as cognitive behavioral therapy or motivational interviewing. These therapies help you learn additional skills to manage your stress and stay motivated for your treatment.
The final stage of addiction and trauma treatment is arranging aftercare to ensure you’re staying committed to your recovery. Your therapist will equip you with the necessary coping skills to handle your triggers outside of treatment, including journaling, breathing exercises or calling a member of your support network. In some cases, you may return for a follow-up session to refresh your memory or deal with new stressors in your life that are causing you trouble.
Relapse prevention planning helps with addiction, providing the tools and support you need to sustain your recovery. You’ll list your triggers and responses during relapse prevention planning with an addiction specialist. For example, if you feel triggered in bars or around friends who drink, you’ll list alternatives you can use to prevent you from relapsing, including meditation, exercising or whatever else works for you.
Relapse prevention planning includes listing members of your support network you can call on when you feel tempted to use substances. These individuals can be friends, family members, your therapist or people from your group therapy sessions.
Trauma is unique to each individual, and their experiences, triggers and responses will likely differ from someone else’s. As a result, multiple types of trauma-informed therapy help individuals overcome their trauma-related issues, including substance use, trauma stress responses and triggers. Different types of trauma-informed therapy also help treat PTSD. Below are the three common types of trauma-informed treatment.
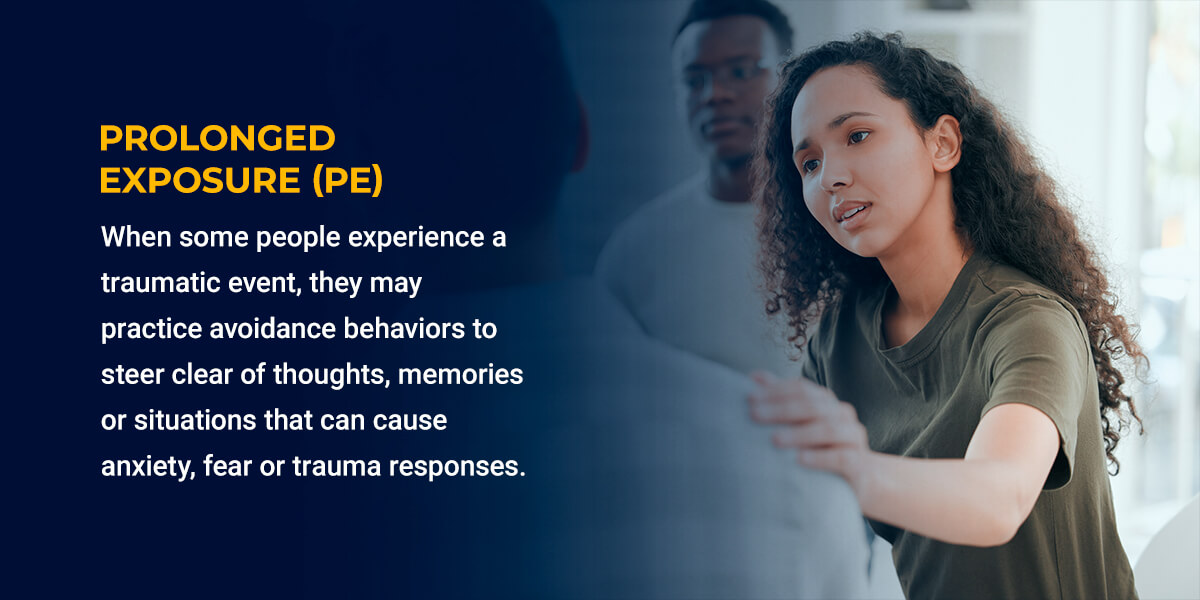
When some people experience a traumatic event, they may practice avoidance behaviors to steer clear of thoughts, memories or situations that can cause anxiety, fear or trauma responses. These avoidance behaviors can impact a person’s life since they may avoid engaging in essential daily or social activities, such as driving, work or relationships. While these behaviors can be seen as an attempt to seek safety or reduce anxiety, they can become extreme and decrease a person’s quality of life.
Avoidance behaviors can worsen trauma stress responses and PTSD symptoms since an individual isn’t addressing their trauma but avoiding it. Avoiding situations that will cause a trauma response is challenging, so it’s beneficial to address your symptoms as soon as possible rather than lessen your quality of life.
PE therapy targets these specific avoidance behaviors by helping individuals confront their fears and anxieties. When a person confronts these fears, anxieties and emotions, they can gradually lessen. The goal is to help prevent a person from using avoidance behaviors and make them feel safe in environments where they once felt threatened.
Different methods of prolonged exposure therapy include:
Prolonged exposure combines the three exposure therapies above, including breathing exercises, psychoeducation surrounding trauma or trauma-informed psychoeducation, talking about your trauma and practicing or confronting your fears in the real world.
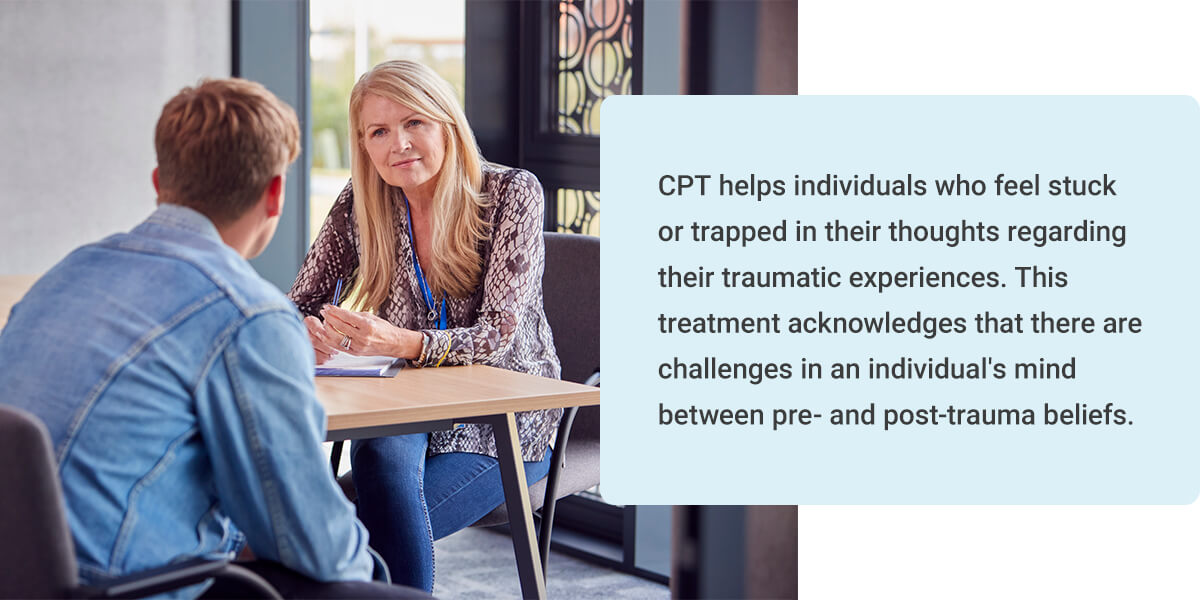
CPT helps individuals who feel stuck or trapped in their thoughts regarding their traumatic experiences. This treatment acknowledges that there are challenges in an individual’s mind between pre- and post-trauma beliefs. For example, a person may have thought they were safe in the world and that nothing bad would happen to them. After their traumatic experience, they may believe everything in the world is inherently dangerous or threatening.
CPT aims to challenge your ideas about why the traumatic event happened and the beliefs you’ve developed after the fact. They can help you address negative thoughts, such as thinking you deserved to experience your trauma or that you’re a bad person and that’s why something happened to you. You’ll learn to change your beliefs to build your confidence, self-esteem and feelings of safety.
CPT also helps you develop coping skills to help you manage your negative beliefs, such as compiling a list of why you might think you deserved to experience trauma and challenging these beliefs with something realistic. You’ll work on these exercises with your therapist, in group therapy or at home.
EMDR utilizes rhythmic left-right (bilateral) stimulation to help people reduce a memory’s impact on their physical, mental and emotional well-being. Focusing on your traumatic memories while using bilateral stimulation enables you to reduce the emotional impact of your trauma, making it easier to process and reducing your response to triggers. The more exposure you have to these memories, the less your negative reaction can be, with the hope of eliminating your negative responses one day.
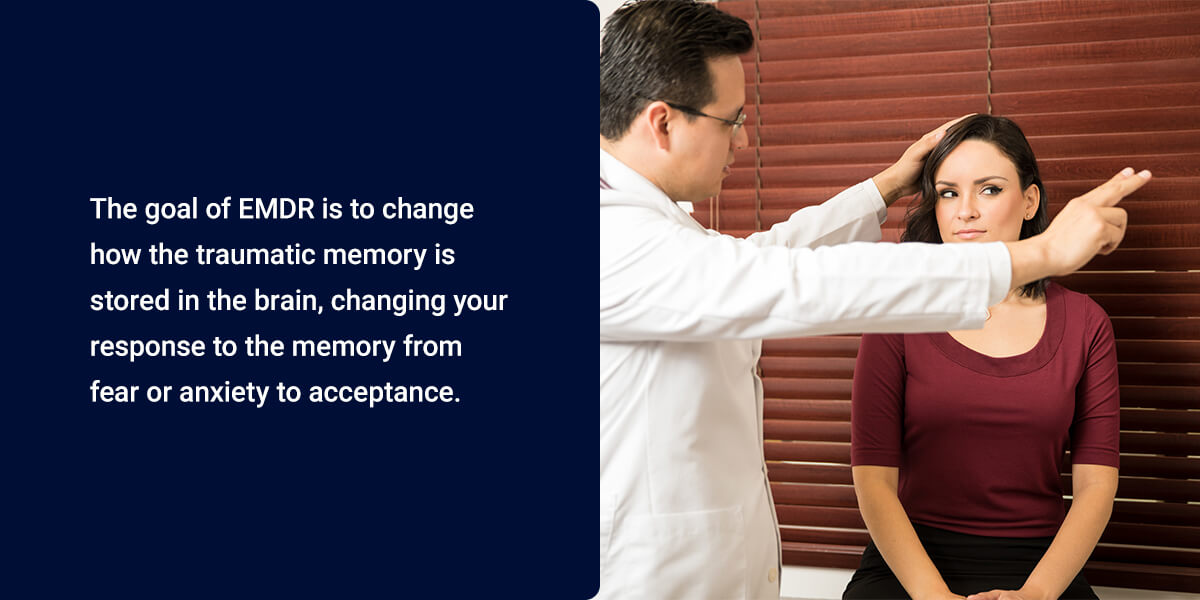
The goal of EMDR is to change how the traumatic memory is stored in the brain, changing your response to the memory from fear or anxiety to acceptance. You’ll also learn how to cope with present and future challenges that may come from triggers or other experiences.
EMDR therapy uses stimulation sets, such as eye movements, taps or tones. Your therapist will ask you to clear your mind and talk about any images, memories or feelings that come to mind as you go through these stimulation sets. You will continue the process until the traumatic memory no longer brings about distress or negative symptoms.
Your therapist may also assign homework for you to complete at home, such as journaling your progress. When you journal, you’ll utilize imagery where you face your fears and visualization techniques to help you imagine a peaceful environment when you encounter a stressful or triggering situation.
A person who has unresolved trauma can experience various physical, mental and emotional signs, including:
Once a person begins using substances to cope, their symptoms may worsen. They can develop sleeping issues, potentially increasing the number of nightmares a person experiences. Their mental health symptoms, such as depression and anxiety, may also worsen, and they may use substances to cope with these new feelings and worsen their unresolved trauma.
Developing a substance use disorder can also isolate you from friends and family, who can be vital members of your support network to help you cope with unresolved trauma. You may start engaging less with activities you once enjoyed, experience problems at work and in relationships or fail to keep up with your daily responsibilities. These effects of substance use can make dealing with traumatic experiences significantly more challenging, which can drive you to turn further to substances.
Rather than relying on substances, seeking help through trauma-informed therapy is recommended. Trauma-informed therapy can work side-by-side with addiction treatment, helping you process and address your emotions and memories associated with your traumatic experiences.
Trauma-informed therapy has many benefits for individuals who have experienced life-altering events. This form of treatment can help you understand your trauma, your responses and how you can change them to improve your life. The following are some trauma therapy benefits:
Trauma-informed therapy can help individuals struggling to cope with their stress symptoms or turning to problematic coping mechanisms to manage their physical, mental and emotional sensations. If you’ve turned to substance misuse to cope with your trauma, Gateway Foundation incorporates trauma-informed therapy into our substance use disorder treatment programs to target the underlying issue and help you reclaim your life.
Leaving trauma untreated can seriously affect a person, especially after long periods. Some of the short-term effects of untreated trauma can cause anxiety and other symptoms, such as:
Many people who go through traumatic experiences may attempt to avoid situations, emotions or thoughts that remind them of the event. These avoidance behaviors can mask the problem and can potentially make their symptoms worse.
If a person leaves their trauma untreated for long periods, they could experience various long-term effects, such as:
These long-term problems can cause significant issues in a person’s life, affecting their health, relationships and mental well-being. A person who starts experiencing the long-term effects of untreated trauma should seek treatment from a therapeutic and addiction specialist.
A person who has gone through a traumatic event may experience trauma responses as they try to go about their day or practice avoidance behaviors, which could prevent them from living fulfilling lives. They may also have difficulty forming and sustaining relationships or experience difficulty keeping up with their daily tasks in fear of exposure to triggering events.
If people turn to substances to cope with their traumatic experiences, their physical and mental health can be impacted even further. Severe addictions can cause numerous health and social consequences, such as:
These substance use consequences, alongside trauma’s physical, mental and emotional challenges, can significantly impact a person’s quality of life. If your or a loved one’s life has been affected by trauma and substance use, it’s time to seek professional help to overcome addiction and address your trauma. Gateway Foundation treats addiction while offering trauma-focused therapy to patients to help them get to the root cause of their addiction and improve their quality of life.
If you’ve never participated in therapy before, especially trauma-focused treatment, you may have some lingering questions. Below we answer some of the most common questions about this therapy.
While you’re addressing your trauma, you’ll likely participate in other types of therapy to help supplement your treatment and help you cope with your experiences. These additional therapies can help you learn the skills and change your current mindset to help you find relief from your addiction and trauma symptoms. The different treatments you may participate in alongside trauma-informed therapy include:
These different therapies can complement your trauma-informed therapy sessions by helping you alter your current mindset, learn additional coping skills, motivate you to stay committed and connect with others who share similar experiences.
While sharing vulnerable information with another person can be uncomfortable at first, it’s beneficial to be honest with your therapist about your experiences so your therapist can help you. You don’t have to worry about the information you share becoming available to anyone else in most circumstances. The Health Insurance Portability and Accountability Act (HIPAA) requires therapists not to share your protected information unless they believe that you or someone else is in danger.
It can be challenging to talk openly with a therapist, especially if you’ve never spoken about your traumatic experiences with anyone before. It can take time to warm up to your therapist, but remember they’re there to help you overcome your challenges and provide the tools you need to improve your overall well-being in a non-judgmental space. Being honest with your therapist as soon as possible helps you get everything you can from treatment and find relief from your traumatic experiences and responses.
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires all insurance providers to cover mental health and addiction services equal to what they would offer coverage for regarding physical conditions. If you have health insurance, you have some form of mental health and addiction coverage.
However, insurance providers are only required to offer coverage for these services equal to what they would provide for physical conditions. So if your coverage for physical ailments is limited, your coverage for mental or addiction services will also be limited.
The good news is that having insurance means at least some of your mental health and addiction services can be covered, saving you from paying for all of your treatment out of pocket. Learn more about Gateway Foundation’s accepted insurance providers.
Explore the latest resources from Gateway Foundation.
We use cookies to give you the best experience on our website. If you continue without changing your cookie settings, we assume that you consent to our use of cookies on this device. You can change your cookie settings at any time but if you do, you may lose some functionality on our website. More information can be found in our Privacy Policy.